

Osteoporosis Treatment: From Diagnosis to Minimally-Invasive Surgery
Most people find out they have osteoporosis after a fall that would not have broken a healthy bone. By then, the disease has usually been progressing quietly for a decade or more. Modern osteoporosis treatment is shifting that timeline — from reactive fracture repair toward early detection and staged intervention, with surgery reserved for the cases conservative care cannot resolve.
Key Takeaways
- Osteoporosis is a progressive loss of bone density that raises fracture risk; a DEXA scan is the standard diagnostic test and can detect the condition years before a first fracture.
- Treatment ranges from calcium, vitamin D, and weight-bearing exercise through pharmaceutical options such as bisphosphonates and anabolic agents, depending on severity.
- Vertebral compression fractures, disc herniation, and spinal stenosis linked to bone loss can often be managed with minimally-invasive endoscopic techniques rather than open surgery.
- Endoscopic approaches typically mean smaller incisions and a shorter hospital stay than open spinal surgery, though recovery still depends on the individual case.
- Coordinated care — imaging, medication, physiotherapy, and surgery when needed under one team — tends to produce better outcomes than fragmented, single-specialty treatment.
Contents
- What Is Osteoporosis, and How Does Bone Density Loss Develop?
- What Causes Osteoporosis?
- How Is Osteoporosis Diagnosed?
- What Are the Main Osteoporosis Treatment Options?
- Can Osteoporosis Be Prevented, Stopped, or Reversed?
- When Is Surgery Needed for Osteoporosis Complications?
- What Is the Recovery Process After Osteoporosis Surgery?
- How Much Does Osteoporosis Treatment and Surgery Cost in Europe?
- FAQ
What Is Osteoporosis, and How Does Bone Density Loss Develop?
Osteoporosis is a condition in which bone tissue loses density and internal structure faster than the body can rebuild it, leaving bones porous and more likely to fracture from minor falls or even routine movements. Bone is living tissue, constantly broken down and rebuilt in a cycle called remodeling. Osteoporosis develops when that balance tips toward breakdown.
The inside of healthy bone looks like a tight lattice — dense, interlocking struts of tissue called trabeculae. In osteoporotic bone, that lattice thins and develops gaps, the way a honeycomb loses structure when too much wax is removed.
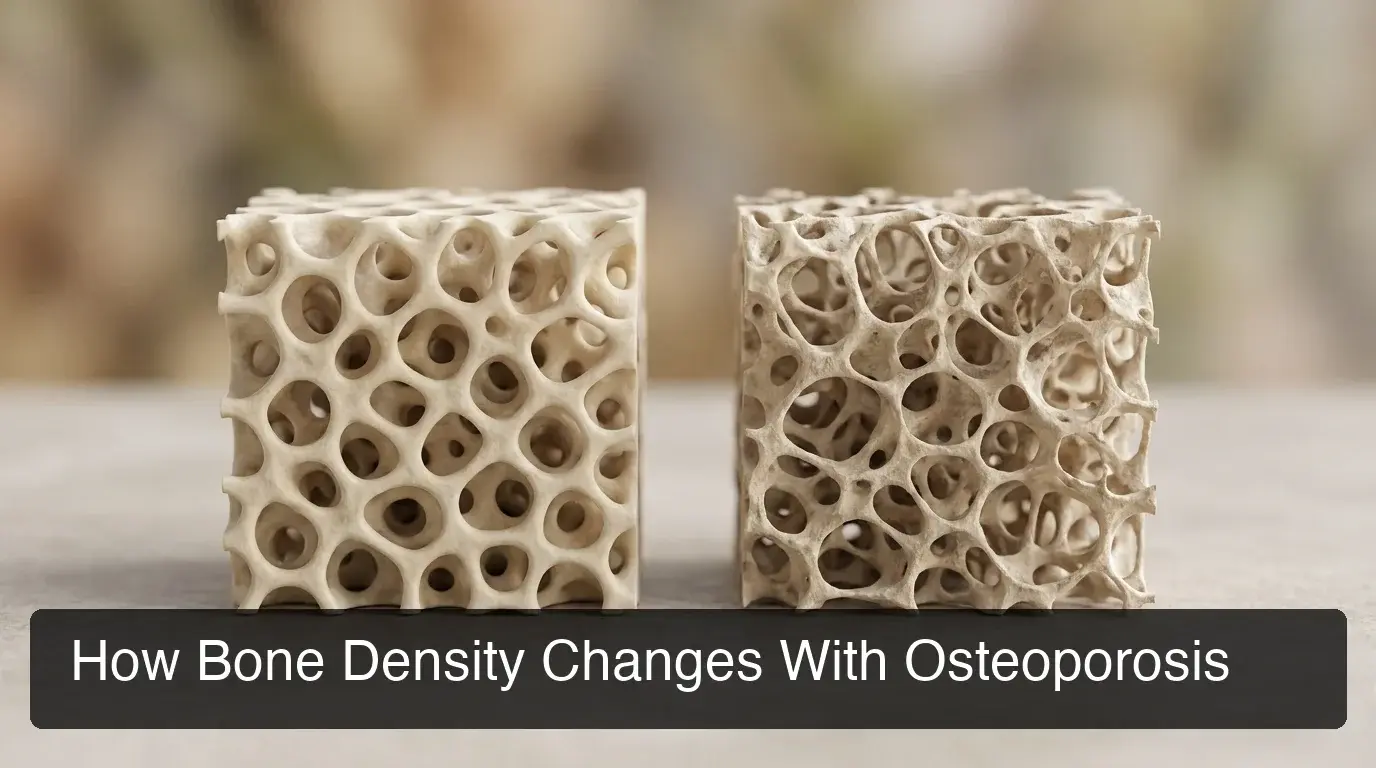
This is why osteoporosis is often discovered by accident. There is no pain associated with density loss itself — the first symptom is frequently a fracture from a fall that a person with normal bone density would have simply brushed off.
What Causes Osteoporosis?
Osteoporosis is caused by an imbalance between bone breakdown and bone formation, driven mainly by aging, declining oestrogen or testosterone levels, and reduced calcium absorption. Genetics, body frame size, and certain medications also influence individual risk.
The most significant driver for women is the drop in oestrogen after menopause, which accelerates bone loss for several years. Men lose density more gradually, tied to the slower decline in testosterone with age.
- Family history of fracture or osteoporosis
- Long-term corticosteroid use for conditions such as asthma or rheumatoid arthritis
- Low body weight or a history of eating disorders
- Smoking and heavy alcohol use
- Thyroid or parathyroid disorders that affect calcium regulation
Worth knowing: Osteoporosis affects men too — roughly one in five men over 50 will experience an osteoporosis-related fracture, though diagnosis in men is often delayed because screening guidelines have historically focused on postmenopausal women.
How Is Osteoporosis Diagnosed?
Osteoporosis is diagnosed using a DEXA (dual-energy X-ray absorptiometry) scan, which measures bone mineral density at the hip and spine and compares it against the density of a healthy young adult. The result is expressed as a T-score, with -2.5 or lower indicating osteoporosis.
A DEXA scan takes around ten to twenty minutes, involves minimal radiation exposure, and requires no injections or preparation beyond avoiding calcium supplements on the day of the test.
Alongside the scan, participants typically order blood tests for calcium, vitamin D, and thyroid function, and may calculate a FRAX score — a ten-year fracture-risk estimate that factors in age, weight, and prior fracture history. Together, these results determine whether lifestyle changes alone are sufficient or whether medication should start immediately.
What Are the Main Osteoporosis Treatment Options?
Osteoporosis treatment typically starts with calcium, vitamin D, and weight-bearing exercise, then adds bone-specific medication — bisphosphonates or anabolic agents — when bone density is low enough to carry significant fracture risk. Surgical intervention is reserved for fractures or spinal complications that conservative treatment cannot resolve.
Bisphosphonates (alendronate, risedronate, zoledronic acid) slow the cells that break down bone, and remain the first-line osteoporosis medication for most patients. For more advanced bone loss, anabolic agents such as teriparatide or romosozumab actively stimulate new bone formation rather than simply slowing loss.

| Approach | How It Works | Typically Used For |
|---|---|---|
| Calcium, vitamin D, exercise | Supports the raw materials and mechanical loading bone needs to rebuild | Early-stage loss, prevention, alongside all other treatments |
| Bisphosphonates | Slows osteoclast activity (the cells that break down bone) | First-line therapy for postmenopausal and age-related bone loss |
| Anabolic agents (teriparatide, romosozumab) | Stimulates new bone formation directly | Severe osteoporosis or high fracture risk despite prior treatment |
| Vertebroplasty / kyphoplasty | Injects bone cement into a fractured vertebra via a needle, under imaging guidance | Painful vertical compression fractures |
| Endoscopic spine surgery | Decompresses or stabilizes the spine through small incisions using a camera-guided approach | Spinal stenosis or disc herniation secondary to bone loss, once conservative care has failed |
By the numbers: The International Osteoporosis Foundation notes that hip fracture risk roughly doubles with each standard deviation drop in bone density — which is why treatment intensity is matched to T-score and FRAX result, not age alone.
Can Osteoporosis Be Prevented, Stopped, or Reversed?
Osteoporosis progression can usually be slowed or halted with early treatment, and some bone density can be rebuilt with anabolic medication — but severely eroded bone rarely returns to its original density. The realistic goal for most patients is stabilizing density and cutting fracture risk, not full reversal.
Weight-bearing exercise — walking, resistance training, stair climbing — bone signals to retain density, in the same way muscle responds to load. Diet matters too: adults over 50 generally need more calcium and vitamin D than younger adults absorb efficiently.
For patients already managing joint or mobility issues elsewhere in the body, knee replacement surgery can restore the ability to walk and bear weight — which in turn supports the bone-loading exercise that slows osteoporosis progression. The two conditions are often addressed together in an older patient’s care plan.
Some patients also explore targeted supplementation as part of a longer-term longevity strategy; KCM’s peptide therapy program covers how these protocols are assessed alongside bone-health goals for patients already tracking their biological age.
When Is Surgery Needed for Osteoporosis Complications?

Surgery becomes necessary when osteoporosis causes a vertebral compression fracture that does not settle with rest and pain control, or when bone loss contributes to spinal stenosis or disc herniation severe enough to compress nerves. These are the complications, not the underlying disease itself, that bring most osteoporosis patients into a surgeon’s care.
Dr. Stanisław Kwiek’s neurosurgical practice at KCM Clinic focuses on exactly this category of case: endoscopic treatment of disc herniation and spinal stenosis, including presentations linked to underlying bone fragility. The endoscopic approach reaches the affected disc or vertebra through a small tubular access point rather than the long incision and muscle retraction required in open spinal surgery.
Two procedures come up most often for osteoporosis-related spinal complications:
- Kyphoplasty or vertebroplasty — bone cement is injected into a fractured vertebra to stabilize it and relieve pain, often performed as a same-day procedure.
- Endoscopic decompression or fusion — used when a herniated disc or narrowed spinal canal is compressing a nerve root, addressing the mechanical problem directly rather than managing pain around it.
Reality check: Not every vertical fracture needs surgery. Many settle with framing, pain management, and bone-strengthening medication over six to eight weeks — surgical review is for cases where pain persists or a nerve is affected.
KCM Clinic runs this decision through its spine and orthopaedic team under EU Medical Devices Regulation standards — the same regulatory framework covering Germany and France — using implant and instrument systems from Zimmer Biomet and Medtronic.
What Is the Recovery Process After Osteoporosis Surgery?
Recovery from minimally-invasive procedures for osteoporosis-related spinal complications is generally measured in days to a few weeks, compared with the extended muscle-healing period that follows open spinal surgery. The smaller access point means less tissue disruption to heal from at the outset.
Kyphoplasty patients are often mobilized the same day, with most discomfort from the original fracture — not the procedure — settling over the following one to two weeks. Endoscopic decompression recovery is longer but still typically shorter than the open-surgery equivalent, since less muscle and soft tissue are cut through to reach the spine.
- Physiotherapy usually begins within the first week to rebuild core and back-support strength
- Bone-strengthening medication continues post-surgery — surgery treats the fracture, not the underlying density loss
- Follow-up DEXA scans track whether density is stabilizing under the revised treatment plan
- Bracing may be used short-term depending on fracture location and stability
KCM’s aftercare package folds physiotherapy, dietetics, and structured follow-up into the surgical pathway, so international patients leave with a plan rather than a discharge letter and a gap.
How Much Does Osteoporosis Treatment and Surgery Cost in Europe?
Osteoporosis treatment costs range widely: ongoing medication and monitoring represent the largest long-term cost for most patients, while a one-off surgical procedure for a spinal complication is typically a larger single payment covered by an all-inclusive package. Costs vary by country, procedure complexity, and whether care is bundled or billed separately.
For UK and Canadian patients used to itemized private billing, a bundled European package — pre-operative assessment, the procedure itself, hospital stay, physiotherapy, and follow-up — is often the more transparent option, since there are fewer separate invoices to reconcile after the fact. Patients considering surgery abroad should compare like-for-like: a headline procedure price that excludes aftercare is not the same as an all-inclusive figure.
Before any bone-density surgery, KCM’s assessment also includes the kind of broader pre-operative health screening used across its surgical programs — the same model applied ahead of procedures like gastric sleeve surgery , where overall health screening before surgery is standard, not optional. Patients traveling for rhinoplasty go through a comparable process, so realistic timeline expectations are set before travel is booked, not after arrival.
Get Coordinated Osteoporosis Care at KCM Clinic
Osteoporosis rarely stays confined to one specialty — it touches endocrinology, orthopaedics, and sometimes spine surgery in the same patient. KCM Clinic coordinates diagnostic imaging, medication review, physiotherapy, and endoscopic surgical care under one multidisciplinary team, with all-inclusive packages built for patients traveling from the UK, Canada, and wider Europe.
Book a Free Consultation with KCM Clinic
Not ready to book yet? Explore KCM Clinic’s full surgical programs — procedure overviews, surgeon profiles, and international patient resources.
FAQ
What does osteoporosis pain feel like?
Osteoporosis itself causes no pain — density loss is silent. Pain appears only after a fracture, most often as sudden, sharp back pain from a vertical compression fracture, or localized pain and swelling after a wrist, hip, or spine fracture from a fall.
What is the best treatment for osteoporosis?
There is no single best treatment; the right approach depends on bone density, fracture history, and overall health. Most patients start with calcium, vitamin D, and exercise, add bisphosphonates or anabolic medication if density is low, and reserve surgery for fracture or nerve-compression complications.
Can osteoporosis be reversed once diagnosed?
Early-stage bone loss can often be stabilized and partially rebuilt with anabolic medication and lifestyle changes. Severely eroded bone rarely returns to its original density, so the realistic treatment goal is usually halting further loss and reducing fracture risk rather than full reversal.
How is a vertical compression fracture treated without open surgery?
Kyphoplasty or vertebroplasty stabilises a fractured vertebra by injecting bone cement through a needle under imaging guidance, without the large incision open surgery requires. It is typically a same-day procedure aimed at relieving pain, restoring vertebral height where possible, and preventing further collapse of the affected bone.
What should you avoid eating or drinking if you have osteoporosis?
Excess alcohol and heavy caffeine intake can interfere with calcium absorption and bone remodeling. Very high-sodium diets also increase calcium loss through urine. None of these need complete elimination for most patients — moderation, alongside adequate calcium and vitamin D, is the standard guidance.
How long does recovery take after minimally-invasive spine surgery for osteoporosis-related fractures?
Kyphoplasty patients are often mobile the same day, with most residual pain resolution over one to two weeks. Endoscopic decompression for stenosis or disc herniation generally involves a longer recovery, but still considerably shorter than open spinal surgery, since less muscle tissue is disrupted during the procedure.






